



















Re-Awakening to Our Inter-connected World
1st International Conference on
Buddhism, Suicide Prevention, and Psycho-Spiritual Counseling
Presentations from Other Countries
Contents:
- Suicide Prevention and “Life-Saving Plus” Networking – Prof. Pum Soo Lee (South Korea)
- Young Adult Suicide among University Students and Buddhist Resources for Meaning in Life – Ven. Huei Kai (Taiwan)
- The Buddhist Spiritual Counseling Model’s Contributions to Mental Care in Hong Kong – Ven. Shi Tianwen (China)
- Applying Mindfulness in the Healing Process – Dr. Prawate Tantipiwatanaskul (Thailand)
- Experienced Applied Buddhist Practices in Psychiatric Treatment for Children and Teenagers – Dr. Chosita Pavasuthipaisit (Thailand)
- Buddhist based Psycho-Spiritual Care for Young Men with Substance Abuse – Ven. Kuppiyawatte Bodhananda Thero (Sri Lanka)
- The Indian Caste System: The Den of Social Suicide – Ms. Pragya Saruchi Chauhan (India)
- Interface of Mental Health in India and Tibetan Buddhism – Ms. Natasha Nair Gupta (India)
- Mindfulness Practice for Being with Suffering & Grief – Prof. Elaine Yuen (U.S.A.)
- Buddhist Chaplaincy & Psychotherapy in Caring for Adolescents & Emerging Adults on the Self Harm-to-Suicide Spectrum – Ms. Jinji Eika Willingham (U.S.A.)
- Christian and Buddhist Synergies in Caring for Those in Pain and Suffering – Rev. Gustav Ericcson (Sweden)
Go to Presentations from Japan
SOUTH KOREA
 Prof. Pum Soo Lee is the Vice President of the Buddhism Counseling Institute of the Jogye Order, Korea’s largest Buddhist denomination. In his talk entitled, Suicide Prevention and “Life-Saving Plus” Networking, he explained how the problem of suicide in South Korea, now the #1 rate in the OECD, is linked to the 1997 IMF financial crisis and the 2007 global financial crisis. These financial crises led to an increase in the gap between rich and poor, intense employment competition, increase in housing prices, and high divorce rates. Such changes in Korean society are shaking up the traditional order and the culture that Koreans have maintained for a long time, such as strong family and group orientations.
Prof. Pum Soo Lee is the Vice President of the Buddhism Counseling Institute of the Jogye Order, Korea’s largest Buddhist denomination. In his talk entitled, Suicide Prevention and “Life-Saving Plus” Networking, he explained how the problem of suicide in South Korea, now the #1 rate in the OECD, is linked to the 1997 IMF financial crisis and the 2007 global financial crisis. These financial crises led to an increase in the gap between rich and poor, intense employment competition, increase in housing prices, and high divorce rates. Such changes in Korean society are shaking up the traditional order and the culture that Koreans have maintained for a long time, such as strong family and group orientations.
Recently, there has been a move toward a social integration model that seeks alternatives to the problems faced by suicide victims in a way different from the previous focus on personal and medical models. In this vein, the activities of the Buddhism Counseling Institute reflect on Buddhist teachings, emphasizing social solidarity and responsibility based on dependent origination and joint karma. This concept of “joint karma” comes from the Yogacara teachings of the Mahayana tradition, which emphasizes the deep interpenetration of life among people living in society or what has been called “interbeing”. The Institute has used this concept to develop a deep Buddhist analysis of the social conditions that lead to suicide. The practice of “joint karma” is to take a Buddhist ethical standpoint to build positive social relations that support the inevitable situation of suffering, which can lead to suicide in societies that have lost their care and concern for social relationships.
From this view, the Institute has developed a wide range of programs based on core Korean Buddhist cultural practices, such as: 1) “suicide psychological” drama, which supports group healing and helps to clarify the value of life; 2) “intergenerational empathy and respect for life” photo-story therapy, which takes an empathic approach to suicide prevention through group sharing; 3) temple stay, which brings the suicidal and also bereaved families together at temples for activities like morning sunrise viewing, group counseling, discussions with monks, dance therapy, image meditation therapy, etc.; and 4) Buddhist memorial services, which support bereaved families.
The Institute has also been training experts in suicide prevention counseling. Most of the existing suicide prevention counseling programs in South Korea have been carried out by adopting modern Western counseling and psychotherapy techniques. However, the Institute has been working with Korean Buddhist universities to develop a training program for specialists in suicide counseling and prevention as part of a Buddhist Counseling College that offers a one-year, three-semester program and a graduate level two-year, four-semester program. Those who receive training will further support and enrich programs the Institute has been running for years, such as: 1) the Jabi Line for Compassion, which started its telephone consultation services in June, 1990; and 2) face-to-face counseling services by Buddhist counseling psychologists and other counseling specialists, who have been visiting elderly welfare centers, nursing homes, social welfare facilities, military installations, juvenile wards, prisons, and suicide victims since 1997.
TAIWAN
 Venerable Huei Kai is the Deputy Abbot of Fo Guang Shan Monastery and a Professor of the Graduate Institute of Religious Studies in the Department of Life-and-Death Studies at Nanhua University in Chiayi, Taiwan. He received his Ph.D. in 1997 from the Religion Department of Temple University in Philadelphia, U.S.A. Ven. Huei Kai often lectures to physicians, nurses, and the general public on life and death, encouraging open discussion on the topic to help individuals come to terms with death, and as a result, have a more fulfilling life. Ven. Huei Kai has released DVDs exploring Buddhist ideas of life and death in the modern world as well as presented Buddhist views on this topic at numerous international religious and inter-faith conferences. He has successfully established the Department of Life-and-Death Studies at Nanhua University, securing the once taboo topic into the realm of scholastic study.
Venerable Huei Kai is the Deputy Abbot of Fo Guang Shan Monastery and a Professor of the Graduate Institute of Religious Studies in the Department of Life-and-Death Studies at Nanhua University in Chiayi, Taiwan. He received his Ph.D. in 1997 from the Religion Department of Temple University in Philadelphia, U.S.A. Ven. Huei Kai often lectures to physicians, nurses, and the general public on life and death, encouraging open discussion on the topic to help individuals come to terms with death, and as a result, have a more fulfilling life. Ven. Huei Kai has released DVDs exploring Buddhist ideas of life and death in the modern world as well as presented Buddhist views on this topic at numerous international religious and inter-faith conferences. He has successfully established the Department of Life-and-Death Studies at Nanhua University, securing the once taboo topic into the realm of scholastic study.
Ven. Huei Kai’s presentation focused on young adult suicide among university students, specifically at his own Nan Hua University, which was established in 1996 by Master Hsing Yun, who founded Fo Guang Shan the largest Buddhist denomination in Taiwan. He began by explaining that suicidal behavior is not so much a response to stress, frustration, and pain in life but rather a failure to face the pressures of life in which frustration and pain lead to the self-mutilation and self-destruction of life. In this way, the best method of prevention and cure is self-awareness of the meaning of life. Only through the inspiration and education of the meaning of life can we truly transform and cure the false understanding and persistence of the life of the suicidal person.
At Nan Hua University, their first step in suicide prevention work was a basic upgrading in physical safety standards such as increasing the height of railings and better controlling access to rooftops. A more comprehensive three level strategy to self-harm was also implemented. Since 2012, the Student Counseling Center has planned and implemented annually a Suicide Prevention Goalkeeper Training Course with different themes to help teachers and students to carry out suicide prevention education programs. These help nurture those qualified teachers and students to become a member of the Gatekeepers within the school and to become an important part of suicide prevention and protection circle on campus. The Center not only sets up a service process for caring for at-risk students who have had suicidal thoughts or attempts, but they also conduct practical exercises on self-harm prevention and control on campus every school year. The school has established a diversified and effective channel of communication through various platforms, such as the Coming of Age ceremony, parent-teacher conferences, a student absence parental contact letter, and at-risk students caring case coordination meetings.
At present, the school employs 3 full-time counselors who are consultant psychologists and 5 part-time counselors who are both professional counselors and clinical psychologists. They assist staff in all departments of the school to implement tertiary prevention (crisis management, referral) and also provide various counseling needs for high-risk and high-care students through both individual consultation and counseling as well as class counseling and group counseling. These measures attempt to improve the students’ crisis conditions caused by psychological problems—such as academic, life adaptation, family, economy and mental status—and at the same time enhance students’ original resilience and life adaptability. At the tertiary prevention level, the Center has also established a cooperation mechanism with community medical resources. In addition to coordinating with the Buddhist based Tzu Chi Hospital in Dalin, physicians of both Chinese and Western medicine are stationed on campus for two hours a week. Nan Hua also works with 27 contracted hospitals to help students with relevant needs to be smoothly referred to suitable medical assistance and treatment.
These activities connect to the University’s core goals of life education, environmental sustainability, intellectual innovation, and the Three Karmic Acts of Goodness (through body, mind, speech). As Ven. Huei Kai emphasized at the beginning, we can only fully transform the tendency towards suicide with a deep education on the meaning of life. In this way, the University has a number of pro-active programs for deepening spirituality and a sense of the meaning of life. For example, they have mindfulness meditation courses on campus during summer break as well as for business people. They believe that through mindfulness meditation, they can help relieve students’ physical and psychological stress and enhance their self-healing ability. They also work with local communities and temples to promote the traditional East Asian Coming of Age Ritual and Ceremony 成年禮 which occurs during university age. Through participating in such a ceremony, students can gain a sense of transformation from an adolescent to an adult who knows how to bear responsibility, be grateful, and cherish life.
HONG KONG, CHINA
 Venerable Shi Tianwen is a Master Lecturer at Tsz Shan Monastery in Hong Kong. He entered the Chinese Buddhist monastic tradition and was ordained as a Buddhist monk in 1996. He has also been studying and teaching Buddhism in Asia and North America. He has received degrees from Cambridge University (M.Phil.) in Educational Research, Monash University (M.Ed.) in Early Childhood Education, and Oxford University (M.Sc.) in Social Anthropology. He also was the Robert H. N. Ho Family Foundation Scholar at Harvard Divinity School’s Buddhist Ministry Initiative program from 2014-15. Since then, he has helped to start the first Buddhist spiritual counseling center in Hong Kong at his monastery.
Venerable Shi Tianwen is a Master Lecturer at Tsz Shan Monastery in Hong Kong. He entered the Chinese Buddhist monastic tradition and was ordained as a Buddhist monk in 1996. He has also been studying and teaching Buddhism in Asia and North America. He has received degrees from Cambridge University (M.Phil.) in Educational Research, Monash University (M.Ed.) in Early Childhood Education, and Oxford University (M.Sc.) in Social Anthropology. He also was the Robert H. N. Ho Family Foundation Scholar at Harvard Divinity School’s Buddhist Ministry Initiative program from 2014-15. Since then, he has helped to start the first Buddhist spiritual counseling center in Hong Kong at his monastery.
In his presentation on The Buddhist Spiritual Counseling Model’s Contributions to Mental Care in Hong Kong, he began by explaining the situation of mental health in Hong Kong. People in Hong Kong are often stressed due to the tremendous working pressure and fast-paced lifestyle prevalent in the culture today. They become anxious when faced with problems in romance, career, finance, health, or interpersonal relationships. They are generally unable to handle these crises and find it difficult to relieve the stress that comes with these challenging periods. When anxiety and stress persist over time, depression, anxiety disorders and other mental issues may arise. These conditions can have a great impact on the daily life of those who are suffering. It may, in some cases, even lead to suicide, self-harm, or violent behavior. With a population of around 7.2 million, it is estimated that 1.7 million people in Hong Kong have mild mental problems; 640,000 have mental illness with moderate severity; and 200,000 have severe mental illness. Hospital authorities estimate that from 2012-2013, adolescents under 17 diagnosed with depression increased by 33% with some cases exhibiting suicidal tendencies. To tackle the current situation before it becomes an endemic public health crisis, Hong Kong urgently needs quality counselling services.
Recently, many western counselling studies have recognized that religion and spirituality are significantly beneficial to mental health. They allow people to understand the meaning of life, maintain an inner happiness and peace, as well as facilitate spiritual growth under the influence of religion and spirituality. Psychologist Viktor E. Frankl, a survivor of the Holocaust, concluded that the meaning of life is the attitude you have while facing adversity. Thus, many counselling treatments have tried to introduce spiritual and religious teachings in order to enhance the effect of treatment. In terms of Hong Kong, Buddhism is one of the six major religions with more than one million followers. Some Buddhist concepts such as “to live in the present moment” and “to let go” are generally well-accepted or even respected among the public. While there is a wide variety of counselling services in Hong Kong, the Buddhist Spiritual Counseling Center established by Tsz Shan Monastery is a pioneer in providing Buddhist spiritual counselling services as part of this prevailing trend. As the core belief of Buddhist teachings is focused on achieving true happiness and peace of mind, people are guided by the Buddhist Spiritual Counseling Model to gain a better insight of their problems through integrating Buddhist wisdom into their daily lives. This counseling system helps free people from their suffering to be able to live a stress-free, peaceful, and harmonious life.
For example, if someone is in emotional distress, facing problems with family, career, or studies, the Center tries to assist through the release of negative emotions, the altering of perspectives towards life’s problems, and the transformation of them into spiritual wisdom, allowing individuals to regain control over their lives through Buddhist insights and teachings. Buddhism provides a method, as much a philosophy or theology, to repair one’s mind through the cultivation of wisdom and knowledge. The Buddhist concept that “everything depends on our mind” is a major feature of Dharma Therapy, where the underlying feeling is addressed before managing the problem itself. As is also known in CBT (Cognitive Behavioral Therapy), the situation itself is not always the problem but rather the perspective of the situation that is the problem. Thus, by changing how you think and feel about the problem, you can completely transform your perspective. Through the counselling service, people rediscover their potential and enhance their personal growth. Dharma Therapy also incorporates the Four Noble Truths and Dependent Origination so that clients come to understand that everything in the world follows the law of cause and effect, which helps them develop a clear direction when they have become disturbed. From the basis of Buddhist practice, the Center helps people to get to “know their mind”, “shape their mind”, and “liberate their mind” to face the ups and downs of life.
Buddhist values and practices are also used to develop the professional staff of social workers and counselors. Going beyond the ethical code and professional conduct of counseling, they develop a view that as all human beings are born with buddha-nature and have the potential to be awakened like the Buddha, each client must be respected individually to discover their own potentials and assets to solve problems. Finally, going beyond support for psycho-therapeutic care for individuals, the Center provides professional training for the helping professions, volunteer training and community education programs, hospital services such as client visits and wellness activities, and finally a range of Buddhist practice programs associated with the main part of Tsz Shan Monastery.
THAILAND
 Dr. Prawate Tantipiwatanaskul received his medical training from Chiangmai University and psychiatric training from Mahidol University, Thailand. He completed his Master of Public Health from the University of Queensland, Australia. Dr. Prawate has trained in mindfulness meditation from three different schools during his psychiatric training and also spent three months as a Buddhist monk in a forestry monastery in Northeastern Thailand. He has been practicing and applying mindfulness in his personal life, his clinical service, and his public education and training programs. In 1999, he published Suicide: Psychological Autopsy and Prevention (Nopburi Printing, Chiangmai).
Dr. Prawate Tantipiwatanaskul received his medical training from Chiangmai University and psychiatric training from Mahidol University, Thailand. He completed his Master of Public Health from the University of Queensland, Australia. Dr. Prawate has trained in mindfulness meditation from three different schools during his psychiatric training and also spent three months as a Buddhist monk in a forestry monastery in Northeastern Thailand. He has been practicing and applying mindfulness in his personal life, his clinical service, and his public education and training programs. In 1999, he published Suicide: Psychological Autopsy and Prevention (Nopburi Printing, Chiangmai).
In his presentation entitled Applying Mindfulness in the Healing Process, he explained how over the past 700 years, Buddhism has become closely tied to the minds of the Thai people and Thai national identity as the traditional “center of Thai education and culture”. Thai Buddhism is distinguished for its emphasis on short-term ordination for every Thai man as a rite of passage into adulthood. Although this is not widely practiced in Thai society anymore, meditation practice has become available to large numbers of Thais since the 1950s, and there are still many influences of Buddhism on Thai people’s way of life and well-being, such as free or donation-based meditation/mindfulness residential programs for the public all year round; books and social media on applying Buddhism in life; networks of Buddhist monks working with local communities and different sectors to reduce suffering and promote well-being.
Concerning the issue of suicide, in the upper northern region of Thailand where the suicide rates has been the highest in the country, Buddhist monks have worked with different groups, especially with the health sector, to prevent suicide. Further, a network of medical professions who provide end-of-life care are trained by a well-known Buddhist monk, Ven. Paisan Visalo, in spiritual care for dying persons. At the same time, persons with mental health problems find respite and seek for “life solutions” through meditation/mindfulness training programs even before they come to see mental health professionals. Further, many of those who have no practice in mindfulness have heard, read, or listened to teachings. The increasing interest of Buddhism and mindfulness practice in the West together with its systematic research help further promote Buddhism as part of a healing process to wider Thai audiences. Many Thai mental health professionals also study Buddhism and practice mindfulness in their personal lives, and many apply mindfulness in their clinical services. In the past, most such professionals have integrated mindfulness in Cognitive Behavioral Therapy, which has now expanded to Mindfulness Based Therapy.
From the biomedical perspective, suicidal depression is an imbalance in brain chemistry. What leads to this imbalance are a number of complex issues more than just biological causes, such as conflicting self-expectations, difficulty expressing emotions, rigid thinking and perfectionism, past unresolved hurts and resentments, anger management, guilt and shame, self-criticism and self-hatred, and hopelessness. In his own clinical work, he teaches basic breathing and mindfulness practices while discussing with patients about its application and continuous learning and practices. Mindfulness and self-compassion in Buddhist teachings can play a significant role in the healing process and provide tools of the therapist. Dr. Prawate finds that his own mindfulness practice is very important in supporting a patient to come back to themselves and become more mindful of internal experiences. They learn to see that behavior is an external expression of an internal state, and that by taking an inquisitive stance to their mind and inner world, they can become aware of strengths and internal resources, which also helps to build self-confidence. In this healing process using mindfulness, one learns to deal with conflicting feelings while getting in touch with psychological needs. In discovering the meaning of one’s suffering, one can learn to cultivate compassion for themselves and others, which allows one to let go of one’s problematic past and find higher meaning in the present. Finally, in his work, he has found studies on happiness as well as positive psychology and brain studies that support his sense of trying to develop positive life goals and action rather than just trying to eliminate one’s negative experiences.
 Dr. Chosita Pavasuthipaisit is a Child and Adolescent Psychiatrist at the Rajanagarindra Institute in Bangkok, Thailand. She has taken extensive practice and training in meditation at various Buddhist centers in Thailand and is also taking training in Anthroposophic Medicine and Anthroposophic Art Therapy, which uses the same principle of mindfulness as in Buddhism. She works specifically with children with mental health problems, especially ADHD, depression, and Anxiety Disorder. With children under the age of eight, she works to apply abstract Buddhist teachings into daily activities, like the mindful use of body movements and separating perception from thought.
Dr. Chosita Pavasuthipaisit is a Child and Adolescent Psychiatrist at the Rajanagarindra Institute in Bangkok, Thailand. She has taken extensive practice and training in meditation at various Buddhist centers in Thailand and is also taking training in Anthroposophic Medicine and Anthroposophic Art Therapy, which uses the same principle of mindfulness as in Buddhism. She works specifically with children with mental health problems, especially ADHD, depression, and Anxiety Disorder. With children under the age of eight, she works to apply abstract Buddhist teachings into daily activities, like the mindful use of body movements and separating perception from thought.
In her presentation entitled Experienced Applied Buddhist Practices in Psychiatric Treatment for Children and Teenagers in Thailand, she first explained the influence of Buddhism on her work. She began practicing Buddhism in her teens through Buddhadasa Bhikkhu, whose teachings go beyond religion and offer a pathway to living and becoming a true human being. She explained that his teachings, however, are quite sophisticated and somewhat abstract, so they are not so easy to apply to children. The most important teacher for her applied work has been Ven. Luangpor Pramote Pamojjo, who has translated the difficult abstract ideas of the Buddhist texts into common Thai expressions that make sense for the young generations. The essence of his teaching can be seen in this quote: “When we become aware of our body and mind and accept the truth of them—that they are impermanent, do not persist, and are beyond control—then we will be liberated and abide in the greatest happiness.” Other important teachers have been: 1) Ven. Paisan Visalo who has been conducting workshops on preparing for death, and his writing in English called “The Seven Factors of a Peaceful Death: A Theravada Buddhist Approach to Death in Thailand”, which was included in the volume Buddhist Care for the Dying and Bereaved (Boston: Wisdom Publications, 2012); 2) Ven. Luangpor Tean, a Thai meditation master who taught movement of the arms while in sitting meditation to develop mindfulness of body movement, a practice that is quite helpful with children; and 3) Chogyam Trungpa Rinpoche, Thich Nhat Hanh, and Rudolf Steiner.
Dr. Chosita then explained how depression is the single largest contributor to the global burden of disease for people aged 15-19, and suicide is one of the three leading causes of mortality among people aged 15-35 (#2 for Thai teenagers). Depression can come in many forms for adolescents, such as sexual problems, behavioral problems, school phobia, attention problems, violence, academic under-achievement, substance abuse, internet addiction, etc. At the Rajanagarindra Institute for Child and Adolescent Mental Health under the Ministry of Public Health, they have created a 24-7 counseling hotline; a set of national Clinical Practice Guidelines for Depression in Adolescents; and a teen clinic for children and teenagers. They also provide web-based counseling practice and psycho-education tools that integrate Buddhist content, such as a smart phone app for youth that helps them work on cognition, coping skills, behavior, positive psychology, assertiveness, and goal setting.
In her clinical practice, a common issue is the relapse of depression after an initial period of taking anti-depressants and entering therapy. This is due to repeated patterns of thinking and feeling, such as loneliness and helplessness, feeling bored of living, and the feeling of something missing internally, which in turn create a chain of developing problems. In this way, medications and psychotherapy alone are not enough to prevent relapses. She noted that using other such standard, modern psychotherapy approaches, like assigned homework, often fail for children and teens. Therefore, she has worked to incorporate Buddhism into her clinical practice. However, since many adolescents are negative about many things, especially religious practices, she has to individually design activities based on a child’s development and specific characteristics. She has been applying Ven. Pramote’s teachings, such as self-observation in which one acts an observer and not a judge which helps in stepping back and getting a distance from usual thoughts and feelings. She teaches practicing mindfulness in daily life, such as, amidst depression, observing moments of happiness, of no feeling, of mindfulness, and of freedom. She also uses separation practices, such as distinguishing between thoughts and perceptions; true perception and distorted perception; and awareness that is different from thinking. Through continual practice, young people can begin to experience how their depression is loosening its control over them. She tries to emphasize the First Noble Truth that their suffering cannot be avoided and must be confronted in order to be transformed. However, this does not work with all young people, so she has developed other practices that are less mental, like mindful coloring or movement (eurythmy), Japanese flower arrangement (ikebana), singing, physical activities outdoors, and yoga for kids.
SRI LANKA
 Venerable Kuppiyawatte Bodhananda Thero is the founder and the Director of the Mithuru Mithuro Movement, the first and the largest Buddhist Rehabilitation Centre in Sri Lanka, where he has successfully rehabilitated more than 5,000 young, male drug addicts in the past three decades. He has established and currently operates five rehabilitation centers around the country and a Leadership Development Center that can accommodate around 100 students and provides outbound training to students as well as professionals. Ven. Bodhananda has successfully adopted and integrated core Buddhist concepts to create a highly effective and a result oriented rehabilitation program. He spends his spare time travelling around the world, educating people on how to harmonize significant Buddhist teachings into their daily existence, and has won more than 30 local and international awards in recognition.
Venerable Kuppiyawatte Bodhananda Thero is the founder and the Director of the Mithuru Mithuro Movement, the first and the largest Buddhist Rehabilitation Centre in Sri Lanka, where he has successfully rehabilitated more than 5,000 young, male drug addicts in the past three decades. He has established and currently operates five rehabilitation centers around the country and a Leadership Development Center that can accommodate around 100 students and provides outbound training to students as well as professionals. Ven. Bodhananda has successfully adopted and integrated core Buddhist concepts to create a highly effective and a result oriented rehabilitation program. He spends his spare time travelling around the world, educating people on how to harmonize significant Buddhist teachings into their daily existence, and has won more than 30 local and international awards in recognition.
He began his presentation on Buddhist based Psycho-Spiritual Care for Young Men with Substance Abuse explaining the situation suicide in Sri Lanka, which was listed as having the 4th highest suicide rate in the world in 2014 by a WHO report. To understand the situation today, one has to reflect on the estimated 100,000 lives lost in the civil war there that spanned over 25 years (1983-2009). From 1985-89, suicide rates were second highest in the world, due to financial hardship, the loss of loved ones, disruption of livelihoods, and mental disorders caused by the war (depression and post-traumatic stress disorder-PTSD). During this time, ideologies of hate and violence were forcefully fed to the minds of the young population, which was a fatal blow to the existing social foundation based on the Buddhist values of non-violence. This change of mindset in the general population initiated a vicious cycle of change in the social structure that continues up to this day. A conflict-ridden history has meant that suicide has become a common method to escape a distressed and psychologically unbearable life. Tackling suicide in Sri Lanka thus necessitates a multifaceted approach.
The most commonly used method of suicide in Sri Lanka today is by pesticide ingestion. The agricultural sector in Sri Lanka represents 31.8% of the national labor force, and they are often subjected to many stressful situations due to finance, weather, workload, and farm related disputes. Suicide amongst farmers is a global phenomenon accounting for up to 300,000 deaths globally per year. Agriculture has the highest rate of mortalities amongst all industries, especially in South Asia. Another at-risk group in Sri Lanka are individuals with a substance use disorder. They are almost 6 times more likely to report a lifetime suicide attempt. Addiction not only increases the likelihood a person will take his or her own life, the disease itself is used as a method of committing suicide. Finally, a new trend in Sri Lanka, which came in to existence with the rapid development in communication infrastructure, has been suicide due to cyberbullying, the inappropriate distribution of pictures/videos over the internet, the use of group suicide sites, and the increase of problematic love affairs formed through social media.
In the year 1987, the Mithuro Mithuro movement began to address the negative shift in Sri Lankan culture as outlined above with activities to help those enslaved by substance abuse under the theme of “Purification through Spirituality”. Their program is especially designed for young men in their teenage years and early 20s. As soon as a resident enters the purification program, he is subjected to an intense screening process to identify any existing psychological conditions that can promote suicidal behavior. From the beginning, he is taught to love and cherish himself, and only then can he start to promote loving kindness towards others. This is done through Buddhist counseling. Since drug addicts are introverts by nature, the program is designed to change that behavior by encouraging the resident to open up about his thoughts and feelings. When he is socialized, he can use the training he received to face any stressful situation with patience. Liberating an individual from drug addiction substantially reduces the risk of suicide.
Four key areas of a human being should be addressed to bring upon a long lasting change: the biological aspect, psychological aspect, social aspect, and spiritual aspect. These roughly correspond to the Buddha’s classical meditation teaching on the Four Foundations of Mindfulness called Satipattana. In the first of these, the Contemplation of the Body (kayanupassana), they work on the rehabilitation of the resident through redeveloping their physical well being and basic physical discipline through meditation and a strict daily schedule that includes cooking and cleaning. The psychological aspect is addressed through the Contemplation of the Mind (cittānupassana), which focuses on peer and group counseling as well as the teaching of Buddhist psychology of the mind and meditation. For the social aspect, connected to Contemplation of Feeling (vedanānupassana), the rehabilitation of social skills and the ability to deal with difficult emotions is emphasized. One important activity in this area is an encounter program where residents are put in a controlled environment to safely express negative or difficult emotions they are having with another resident. There is also a program that focuses on family reconciliation. The final, spiritual aspect or Contemplation of Dharma (dhammanupassana) involves the development of the personality towards a religious or spiritually desired better personality. As a Buddhist organization, they focus on providing a good understanding of core Buddhist concepts, such as the Five Precepts, Dependent Origination, the Four Noble Truths, and the Noble Eightfold Path, which provide a practical grounding for integrating the other three areas of development.
As residents continue to develop, they are given increasing responsibility within the community, becoming mentors to new residents and eventually gaining the chance to join the movement as staff. In this way, the program is not run as a professional organization with staff brought in from the outside, but rather as a community whose members are all in various stages of purification and practice.
INDIA
 Pragya Saruchi Chauhan works as a software engineer, but feels that she was not born to be one. She discovered her love and passion in psychology. From her adulthood onwards, she has become very keen in observing people, their behavior, and why everyone is so different. Meditation and the Buddha’s teachings have taught her why some are suffering and some are happy. She has studied Neuro-Linguistic Programming (NLP) from the American Union of NLP and in parallel is completing a Masters in Psychology. This has given her a larger perspective of humans as individuals alone, in groups, and in social contexts, and has taught her how we perceive the world filtered by our experiences, beliefs, values, and assumptions rather than the real world.
Pragya Saruchi Chauhan works as a software engineer, but feels that she was not born to be one. She discovered her love and passion in psychology. From her adulthood onwards, she has become very keen in observing people, their behavior, and why everyone is so different. Meditation and the Buddha’s teachings have taught her why some are suffering and some are happy. She has studied Neuro-Linguistic Programming (NLP) from the American Union of NLP and in parallel is completing a Masters in Psychology. This has given her a larger perspective of humans as individuals alone, in groups, and in social contexts, and has taught her how we perceive the world filtered by our experiences, beliefs, values, and assumptions rather than the real world.
In her presentation entitled The Indian Caste System: The Den of Social Suicide, she explained the basic nature of the Indian caste system as derived from the mythic varna system of early Vedic Hinduism. Those who were formerly called Untouchable, a status made illegal only in 1955 under the post-independence Indian constitution, are now called Dalit, a rather pejorative term that means “oppressed” or “broken/scattered” people. Although the practice of discrimination based on caste was legally outlawed, it still exists in numerous cultural customs and permeates through most of India’s institutions, such as government, press, universities, businesses, etc.
Pragya focused her talk on the recent incidents involving caste-based discrimination on Indian university campuses that have led some Dalit students to commit suicide. In general, India has one of the world’s highest suicide rates for youth aged 15 to 29. In 2015, the number of student suicides in India was 8,934. The number of attempted suicides, many unreported, is likely to be much higher. Every hour, one student commits suicide in India, according to 2015 data from the National Crime Records Bureau (NCRB). The causes for suicide have been attributed to various sociological, psychological, biological, and environmental factors. There is a strong correlation between low educational achievement, poor performance in examination, stress, and attempted suicide among students. However, other reasons for distress among students that have been identified are: the impact of recession, financial problems, family problems, social exclusion, and caste discrimination. Studies show that Dalit students have higher suicide rates compared to others. The context behind these suicides is failure, the fear of failure, administrative indifference to their situation, hostile regulations, insults, and social and academic stigmatization and rejection. Dalit youths unable to face institutional and structural discrimination end up committing suicide due to the social and psychological exclusion they experience.
One of the most jarring incidents is the case of Rohith Chakravarti Vemula who was a PhD student at the Central University of Hyderabad. His suicide on January 17, 2016 sparked an outrage throughout India, highlighting the cases of systemic discrimination in educational campuses across India. The 26-year-old hanged himself the day after he and four other students were suspended by the university and were barred from their hostel. His death occurred after a controversy, which extended over several months starting in July 2015, when the university reportedly stopped paying him a fellowship (US$390) per month after he was found “raising issues of Dalit humiliation on the campus” through his book Caste is Not a Rumor. There was considerable pressure from at least two major politicians on the university to punish Vemula and other Dalits. An open letter was written to the Vice-Chancellor of the University of Hyderabad by over 220 worldwide academics “expressing their shock and anguish” at Rohith Vemula’s suicide.
In Vemula’s final note, he expressed some of his feelings as, “The value of a man was reduced to his immediate identity and nearest possibility. To a vote. To a number. To a thing. Never was a man treated as a mind. As a glorious thing made up of star dust. In every field, in studies, in streets, in politics, and in dying and living … My birth is my fatal accident. I can never recover from my childhood loneliness. The unappreciated child from my past.” Pragya then explained how Emile Durkheim’s theory of suicide as a structurally conditioned social fact has been extremely important in understanding that suicide is not an individual act, but rather a social and political act towards the structure of the society that contributes to it. Before Durkheim, suicide had been generally considered at its individual or psychological level. It was Durkheim who first scientifically studied suicide as a social fact. Pragya explained that it is an unambiguous fact that Rohith Vemula was victim of both explicit and implicit forms of caste-exclusion that have been ongoing in Indian universities. Suicide as a social and political act is the most remarkable theme that emerged as the aftermath of Rohith’s suicide. For such suicides to end, social inequality must also end.
Shortly after Durkheim died in 1917, Dr. B.R. Ambedkar, a Dalit leader and the architect of the post-independence Indian Constitution, began his social campaigns to eradicate social inequality and caste-based violence in India. By 1956, he had accomplished much on the legal front but felt the mentality of caste still permeated Indian society. Thus, turning his back on what he felt was the source of this mentality in Vedic Hinduism, he converted to Buddhism at a grand ceremony in Nagpur in October 1956 along with half a million Dalits. Dalits and other “refugees” of this caste mentality, which is also rife with patriarchy, have since embraced Dr. Ambedkar’s understanding of Buddhism as a social revolution that helps people to cultivate a higher sense of self-esteem, develop confidence, and change one’s relationship with oneself and others. Although Vemula as a social activist had not embraced Buddhism personally, his mother and brother embraced it shortly after his death on the occasion of Dr. Ambedkar’s 125th birth anniversary on April 14, 2016.
Pragya concluded by explaining her developing activities in organizing youths throughout India to respond to the psychological wellbeing of the oppressed communities. As caste is a psychological notion that manifests in graded interpersonal exchanges, understanding the psychology of caste is an important aspect to transforming daily social interactions. Witnessing the many brilliant Dalit students committing suicide at premier Indian universities, she took the initiative to started an online counselling group for people going through such psychological challenges. She also belongs to the Nagpur Collective, a national network of young scholars, activists, students, academics, and professionals from the Ambedkar Buddhist tradition working on caste-based violence, including suicide among Dalit people.
 Natasha Nair Gupta is an integral psychotherapist in private practice in New Delhi. She was trained at the California Institute of Integral Studies (CIIS) in San Francisco. CIIS is a pioneer in transpersonal studies and was the first to offer a transpersonally-oriented, East-West psychology program in the world. Subsequently, she trained in Peter Levine’s Somatic Experiencing (SE) in Europe. SE aims at resolving health problems related to mental, emotional, and physical trauma by focusing on releasing the trauma shock stuck in the body. Natasha is also trained in Raja Selvam’s Integral Somatic Psychotherapy (ISP), which is an advanced approach for integrating body, energy, and consciousness into any psychological process.
Natasha Nair Gupta is an integral psychotherapist in private practice in New Delhi. She was trained at the California Institute of Integral Studies (CIIS) in San Francisco. CIIS is a pioneer in transpersonal studies and was the first to offer a transpersonally-oriented, East-West psychology program in the world. Subsequently, she trained in Peter Levine’s Somatic Experiencing (SE) in Europe. SE aims at resolving health problems related to mental, emotional, and physical trauma by focusing on releasing the trauma shock stuck in the body. Natasha is also trained in Raja Selvam’s Integral Somatic Psychotherapy (ISP), which is an advanced approach for integrating body, energy, and consciousness into any psychological process.
In her presentation entitled the Interface of Mental Health in India and Tibetan Buddhism, she explained that India is a diverse country with many subcultures within cultures, so it is difficult to make generalizations about mental health. However, one can note these basic points: India has a higher suicide rate at 15.7/100,000 (2015) than the global average (10.6) or even the regional average (12.9). It is found to be the leading cause of death among those aged 15-29 in India; causes about twice as many deaths as HIV/AIDS; and is on par with maternal causes of death for young women. Further, mental illness is growing in India. The proportion of all burdens explained by mental, neurological, and substance use disorders rose from 3% in 1990 to 6% in 2013. As of 2015, 50 million Indians suffer from depression and 30 million from anxiety, and these are only the reported cases. It is estimated that 50% of cases go unreported because of the fear of social stigma attached to having a mental illness.
Most Indians have limited access to care for mental illnesses. There is a lack of community and support services for the prevention of suicide. Further, there is a social stigma attached to mental illness, because of the ignorance around it. There is a shortage of skilled professionals with only 3,000 psychiatrists for an estimated requirement of 11,500; 500 clinical psychologists for an estimated requirement of 17,250; and 400 social workers who can work with patients with mental illness when the need is for 23,000. The additional problem is that most of the mental health professionals in India are informed by the medical model, which focuses on symptom alleviation or behavior modification as opposed to deeper personality change and growth. The humanistic paradigm has a more holistic view of human nature and views symptoms as messengers of disharmony in an individual. The field has evolved further still, with the newest paradigm of Transpersonal and Integral Psychology, wherein common mental disorders are even viewed as opportunities to wake up. These traditions believe that for mental health not only is the absence of disease important, but also the presence of something else—of individuals being connected to a deeper and larger truth about themselves and the universe.
In this vein, Natasha highlighted how the Tibetans in exile in India and Bhutan have managed to revive and preserve the sophisticated Buddhist tradition across hundreds of monasteries. They offer an extensive and advanced tradition of study and training of the mind and emotions, with a wide array of methods to transform emotions and consciousness at the deepest level. Because of this, it is felt that Buddhism can play a significant role in working with common mental disorders like anxiety and depression. Natasha’s own teacher, Dzongsar Khyentse Rinpoche, the teacher and founder of the Deer Park Institute in Bir, India, is seeking to help further bridge this gap between modern psychology and the wisdom traditions of Asia. He has three monastic institutions in India and Bhutan under his spiritual guidance. Under his guidance, they are working towards creating a curriculum to train monastics in mental health.
The project based out of Deer Park has a number of potential strengths. In India and Bhutan, where spirituality is an integral part of the lives of common people, there might be more openness to seeing a person in robes than to a psychologist. Monasteries are often located in remote areas which could prove invaluable as there is little or no availability to mental health services outside of big cities and towns. There are already thousands of monks adept in working with transformation of the mind and emotions. By familiarizing them with psychological terminology, understanding the developmental perspective and integrating the findings of what has been found to be most therapeutic in working with mental illness, there is potential for access to a quick “work force” in place. Since the desire to help comes from a sense of compassion instead of remunerative gain for monastics with less material needs, it will be much more affordable to people. She concluded by noting that their effort to bring together the psychological and spiritual by training monks to work in mental health can go further than just treating symptoms but can work at the root of our problems—ignorance. In doing so, this will make a small step towards sustainable peace and happiness in the world.
U.S.A.
 Elaine Yuen is an Associate Professor of Religious Studies and Chair of the Master of Divinity Program at Naropa University in Boulder, Colorado where she teaches courses on spirituality and ritual, Buddhism, and pastoral care. She has taught national and international programs exploring the interfaces between Buddhism, meditation, creativity, and contemplative care-giving. Prof. Yuen is cross-trained as a social science researcher and is particularly interested in the relationship between meditation and the creative process. A Senior Teacher in the Shambhala Buddhist tradition, founded by Chogyam Trungpa Rinpoche in the early 1970’s, she continues her exploration of contemporary life through many activities as a teacher, parent, and artist.
Elaine Yuen is an Associate Professor of Religious Studies and Chair of the Master of Divinity Program at Naropa University in Boulder, Colorado where she teaches courses on spirituality and ritual, Buddhism, and pastoral care. She has taught national and international programs exploring the interfaces between Buddhism, meditation, creativity, and contemplative care-giving. Prof. Yuen is cross-trained as a social science researcher and is particularly interested in the relationship between meditation and the creative process. A Senior Teacher in the Shambhala Buddhist tradition, founded by Chogyam Trungpa Rinpoche in the early 1970’s, she continues her exploration of contemporary life through many activities as a teacher, parent, and artist.
In her presentation entitled Mindfulness Practice for Being with Suffering & Grief, she first spoke about issues concerning how we connect as caregivers through empathy and compassion. In empathy, which is putting oneself in the position of another, there is the problem of over connecting and getting too involved with the client’s suffering (empathic contasion) or disconnecting and withdrawing from the client’s suffering (emotional disengagement). Compassion is the act of reaching out to assist someone else in pain. In the neurological world, it has been shown this act of reaching out supports the development of pro-social neural networks that increase our ability to care for others. However, there is also what is called “compassion fatigue”, which is the stress response from caring when there are no expected rewards, results, and often closure. This fatigue often results in a diminished capacity for empathy and interpersonal engagement.
Clearly, mindfulness supports all the different practices in developing compassion as well as helping a person be aware of the struggles in holding and dealing with another’s pain. There is a great detail of research evidence on mindfulness that says it helps with emotional regulation and improved attention, producing greater calm and stress reduction as well as enhanced coping skills. Mindfulness not only calms the mind, but also helps one become more aware or attuned to signals in the body which may arise before they do in the mind or heart.
These days there is increasing research into what is called self-compassion. Mindfulness has an important role in this practice by helping counter over-identification and fixation on negative thoughts. When we encounter suffering, there are different aspects of our psychology that we can use to enable us to care for ourselves as we care for others. These are: finding the right balance in engaging with others (emotional attunement), coming to understand and appreciate the unique vantage points of others and understanding the larger context (cognitive attunement), and developing congruence in goals and values between clinicians, patient, and family (moral attunement).
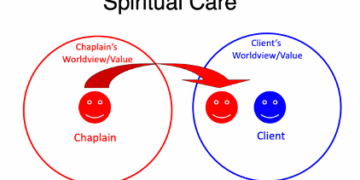
Prof. Yuen then went on to discuss pastoral care education, specifically the training in religious and Buddhist practices for caring, at Naropa University. She described three lenses of pastoral care: 1) premodern or traditional: care accessed through religious rituals, traditions, and spiritual experiences; 2) modern: care that includes rational and empirical knowledge, such as psychology and medical science, and 3) postmodern: care that is aware of and addresses contexts such as cultural and social identity. Although the core of Naropa’s curriculum is focused on Indo-Tibetan Buddhism, they do have students from other Buddhist and religious traditions. Students are required to practice meditation five hours per week, participate in a practice week during the semester, and complete a one-month retreat before graduating the program. The emphasis is on inter-faith care, because the United States has such religious diversity. This has two aspects: one is to be grounded in one’s own meditative or contemplative practice so that one can be present and open with patients from a variety of different backgrounds; the other is that patients from other traditions may require or wish to have certain forms of basic religious services performed for them, and the chaplain must be able to respond accordingly. Students are also trained to not just work in hospitals but to also respond to a variety of care environments they may enter such as in prisons or the military.
Finally, Prof. Yuen spoke about overall Buddhist Ministry Education in the United States. For the last three years, there has been an annual gathering of the Buddhist based Masters of Divinity and Buddhist ministry education programs, which has included Naropa University, Upaya Zen Center, New York Zen Center for Contemplative Care, Institute of Buddhist Studies, Harvard University Divinity School Buddhist Ministry Initiative, and others. Discussion topics have included: how their Buddhist training programs might (or might not) appropriately meet the professional standards for service that are often rooted in Western paradigms; what is right livelihood or the means of making a living for Buddhist teachers and practitioners; what are common Buddhist theological foundations; what are the particular Buddhist epistemologies or ways of knowing; what is the common ground they share as Buddhist institutions and faculty?
 Jinji Eika Willingham is a clinical psychotherapist and Zen Buddhist hospital chaplain at South Austin Medical Center where she works with patients, families, and teaches self-care and mindfulness practice to medical caregivers. She is a Zen practitioner at Upaya Zen Center in Sante Fe and Plum Blossom Sangha in Austin, and founder of Stage of Life Counseling and Contemplative Care. In her clinical practice with individuals, couples, parents, and families, she specializes in full-spectrum trauma (relational, systemic, crisis), PTSD, grief and loss, life transitions, mood disequilibrium, depression, and anxiety. She has a B.A. in History, an M.A. in Intellectual History, a C. Phil. in English (UCLA), and an M.A. in Counseling Psychology. She is presently completing her chaplaincy training towards her M.Div. at Upaya Zen Center in Sante Fe under the guidance of Roshi Joan Halifax. Her thesis presents an integrated clinical model of dharma-therapy called ENSO Psycho-Spiritual Care.
Jinji Eika Willingham is a clinical psychotherapist and Zen Buddhist hospital chaplain at South Austin Medical Center where she works with patients, families, and teaches self-care and mindfulness practice to medical caregivers. She is a Zen practitioner at Upaya Zen Center in Sante Fe and Plum Blossom Sangha in Austin, and founder of Stage of Life Counseling and Contemplative Care. In her clinical practice with individuals, couples, parents, and families, she specializes in full-spectrum trauma (relational, systemic, crisis), PTSD, grief and loss, life transitions, mood disequilibrium, depression, and anxiety. She has a B.A. in History, an M.A. in Intellectual History, a C. Phil. in English (UCLA), and an M.A. in Counseling Psychology. She is presently completing her chaplaincy training towards her M.Div. at Upaya Zen Center in Sante Fe under the guidance of Roshi Joan Halifax. Her thesis presents an integrated clinical model of dharma-therapy called ENSO Psycho-Spiritual Care.
In her presentation entitled Buddhist Chaplaincy & Psychotherapy in Caring for Adolescents & Emerging Adults on the Self Harm-to-Suicide Spectrum, she explained that she did not set out to specialize in clinical work with young adults but that they’ve wound up seeking her out as a therapist. While she does have clients who are actively suicidal, many of her clients are slowly killing themselves in other ways, through a spectrum of self-harming behaviors: abusive relationships and a variety of addictions, such as alcohol and drugs, technology, hoarding, gambling, eating, exercise, sex, danger, porn, etc. In the Realm of Hungry Ghosts written by Gabor Maté—a Hungarian born Canadian physician working in childhood development and trauma—he makes a compelling exploration of addiction as the result of insecure attachment, the opposite of which is positive connection. She has not been surprised to see this very represented in her clinical population, as many of her clients have experienced family abuse and relational trauma that have impaired their ability to emotionally regulate, cognitively reframe, and care for themselves. Such relational harm calls for interpersonal healing as a “positive disconfirming experience” or relational repair work through her psycho-spiritual clinical model.
Buddhist teachings offer accessible metaphors that provide her clients with meaning, validation, and support in the process of exploring, enduring, and transforming their relationship to their own suffering. In addition to the metaphors of “no mud, no lotus” (which conveys that we must do our own “composting” in life) and “remove the second arrow” (which involves seeing and then discontinuing secondary suffering), she often shares the story of a young man who left home, engaged in extreme behaviors such as self-harming, becoming virtually anorexic, and nearly dying. Then she tells them that this young man went on to become the Buddha and that the process of sitting down and bearing witness to his own suffering—the first step of the Four Noble Truths—led to his awakening. Presenting the Buddha as a secular historical figure, young adults begin to recognize themselves in the Buddha’s initial destructive behavior and are startled to also see the courageous vulnerability and awakened spirit of the Buddha in themselves.
Willingham also spoke about Buddhist chaplaincy as the foundation of Dharma-Therapy by introducing some of the work of her teacher Rev. Joan Halifax. One of Rev. Halifax’s most compelling training tools, which she has started to teach in Japan, is called G.R.A.C.E. This is a secular contemplative practice based on the Satipattana Sutta of the Four Establishments of Mindfulness. It was first developed by Rev. Halifax for medical caregivers who work with the seriously ill and dying in hospitals and hospices, but Willingham shares this with a wide spectrum of caregivers including other psychotherapists, teachers, parents, social workers, and social justice advocate in addition to medical professionals at the hospital. The practice of G.R.A.C.E. begins within the caregiver by Gathering attention, Recalling intention, and Attuning to self (sensory/somatic, affective/emotional, cognitive). It then leads outward in Attuning to others, Considering what will best serve—what is the appropriate or compassionate action—and finally into Engagement, the appropriate action. These skills are of critical importance to caregiver self-care and constitute an ethics of care, because they allow the caregiver to distinguish between empathy (over-identifying with the client) and compassion (care that serves, and also nourishes and does not fatigue the caregiver). G.R.A.C.E. supports both compassion and equanimity—expressed by Rev. Halifax as work with a “soft front and strong back,” as well as offering care that is not attached to outcome—something that is vital in working with self-harming/suicidal clients, Willingham pointed out.
Another essential point Willingham made about Dharma-Therapy is that it shares viewpoints with both western Systems Theory (interdependence) and Buddhist teachings (interdependent co-arising) like that found in the Prajnaparamita Heart Sutra. Because everything is an aggregate, comprised of things other than itself, “everything is everything,” and is highly relational. Everything is a product of “we” (wherein 1+1 = 3), and is always shared, dynamic, and emergent.” Applying this to psychotherapy, Willingham emphasized that the non-separate relating and the shared nervous system of those in the room is what allows the psychotherapist to help regulate dys-regulated clients. By supporting clients’ relationships to somatic experience (bodily sensation), affective experience (emotions), and cognitive experience (thoughts), relational work builds and sustains the container for courageous excavation of past fragments, exploration of ideas (both positive and negative), and present experience, resulting in self-compassion, resilience, adaptive growth, and maturation.
Several relatively recent models of psychotherapy emerging in the West are congruent with and/or are using Buddhist ideas, such as Mindsight, Attachment-based Interpersonal Neurobiology, Internal Family Systems Therapy, and Somatic Experiencing. Each provides different ways for clients to turn towards what hurts and de-identify with their suffering by titrating and oscillating to build distress tolerance and return to a regulated baseline. In conclusion, she remarked that Buddhist chaplains and practitioners would benefit from knowing more about counseling and therapy, while psychotherapists would benefit from knowing more about the foundations of Dharma and Buddhism so they do not practice a reductive notion of mindfulness as a spiritual bypass model of “just breath, be calm, and smile.” This non-separate clinical approach is the impetus for her development of Dharma-Therapy into an integrated model of psycho-spiritual care.
SWEDEN
 Rev. Gustav Ericsson is a Christian priest in the Lutheran Church of Sweden. After being ordained in 2010, he served as a hospital priest at the regional University Hospital of Umea in northern Sweden and at a hospice for palliative care. He is especially trained in pastoral counseling for crisis and grief, and one of his main interests is the meeting of meditation practice with pastoral care. He has practiced and studied Zen since the mid 1990’s and in 2004 received Dharma transmission from Japanese Soto Zen teacher Gudo Nishijima Roshi. Since 2010, he has also served as a counseling priest with the Lutheran Church’s national suicide prevention hotline, which is available by telephone through the national emergency number as well as chat rooms and mailbox online.
Rev. Gustav Ericsson is a Christian priest in the Lutheran Church of Sweden. After being ordained in 2010, he served as a hospital priest at the regional University Hospital of Umea in northern Sweden and at a hospice for palliative care. He is especially trained in pastoral counseling for crisis and grief, and one of his main interests is the meeting of meditation practice with pastoral care. He has practiced and studied Zen since the mid 1990’s and in 2004 received Dharma transmission from Japanese Soto Zen teacher Gudo Nishijima Roshi. Since 2010, he has also served as a counseling priest with the Lutheran Church’s national suicide prevention hotline, which is available by telephone through the national emergency number as well as chat rooms and mailbox online.
In his presentation on Christian and Buddhist Synergies in Caring for Those in Pain and Suffering, he explained that in the Bible, there are several suicides mentioned along with other passages describing suicidal thoughts and feelings. For example, Saul in the First Book of Samuel (31:4) falls on his own sword, and Judas in the Gospel of Matthew (27:5) hangs himself. Generally speaking, suicide has been regarded as a sin in much of the history of the Church. It has been considered a violation of the commandment not to kill and to be an act against the Will of God. For hundreds of years, for example, the body of a person who had taken his or her own life was not allowed to be buried in the churchyard. While some streams of Christian theology unfortunately still uphold various versions of this kind of idea, he is glad to report that many Church traditions have changed. The Church of Sweden has not made any formal statement regarding suicide, but the closest thing to an official statement is found on its website: “The Book of Job (1:21) says that only God has the right to give and take human life. However, the Bible also says that neither life nor death, angels or evil spirits, can separate us from God’s love.”
The Lutheran Church of Sweden has a suicide helpline that started in 1956 in a town called Kristianstad with an ad in the local newspaper that said: “Before your take your life, call this number.” Other cities and church dioceces followed example, and with time the church’s helpline became available all over the country. When the local helplines were joined together into one national service, a cooperation with the 112 national emergency phone number was initiated. For many years now, priests from all over the country log on to the same service, and callers are connected through the 112 operators. The priests in the helpline are both male and female, and he has been one of the helpline priests since 2010. The training before their ordination includes relevant theological studies as well as pastoral counseling practice. Sometimes counseling training is with an actor that provides challenges in a realistic situation, which is then discussed in the group. Also, they have all completed an introduction to working in the suicide prevention service held by their respective diocece, and the training for the helpline priests is also ongoing.
From a faith and practice perspective, he has learned three things that have helped him when meeting difficult situations regarding suicide and grief counseling. The first is to practice being a walking prayer room, which means acting as or providing an open and welcoming space with many possibilities. To meet someone as a prayer room is to offer space, time, and presence, and not having all the answers. The second is to walk slowly in the hospital corridors. The way he walks, as well as the way he talks, should represent something else than the stress and anguish of those he meets, including other caregivers. The third is to enter every room with empty hands, which means letting go of ambitions and ideas about what he should say and do as well as emptying himself in order to be able to receive the people and the situation that he meets in the room. These three principles as well as seeing the Christ that is already here and releasing the weight are all to a large extent upheld and nourished by his practice of sitting meditation (zazen) and walking meditation (kinhin). The sitting and walking of Zen meditation has become part of the nucleus of his service as a Christian hospital priest. In his experience, it is deeply helpful, and he is very grateful for the privilege to continue his meditation training.
Return to Conference Overview